
| Search Home Find us Feedback |
 |  |
Information for children, teenagers and families | |
Problems that might (or might not) happenProblems are listed alphabetically, not in likelihood of them happening! Allergic Broncho-Pulmonary Aspergillosis - ABPAAspergillus is a fungus (the same thing as a mould) which is found everywhere, but especially in rotting vegetation and dust. Aspergillus releases millions of invisible spores into the air that we all breathe in every day. Most of the time the spores cause no problem, even if they start to grow in the airway mucous. Very occasionally the body can make an allergic reaction to the Aspergillus growing in the airway and this response called ABPA (allergic bronchopulmonary aspergillosis). The allergic reaction irritates the airway and can give exactly the same symptoms as a chest exacerbation caused by infection with increased cough and loss of lung function. ABPA can also cause wheezing. ABPA can happen at any age. We need to think about it and test for it when children have chest exacerbations that don't get better with antibiotics or which comes back quickly or if children are wheezy. The main test for ABPA is to measure the allergy antibody level (IgE) in the blood. Sometimes we will also do a chest X-ray. The treatment for ABPA is to dampen down the allergic reaction with steroid medicine (prednisolone see medicines section), which needs to be taken for several weeks, and which can have some unwanted side-effects. If the cough swab or sputum samples have grown Aspergillus, we will also use an anti-fungal drug called itraconazole. See the 'bugs' page for more information about Aspergillus. Bowel blockage - distal intestinal obstruction syndrome (DIOS)
Detecting early DIOS and treatmentIt is sometimes possible to feel that the last part of the small intestine is thicker than it should be, and this is one of the reasons we feel the tummy children come to clinic. We often call this a 'right iliac fossa mass'. This can go on to cause partial or complete bowel blockage. When we feel this mass, we will recommend treatment using movicol. This is a special drink which makes the contents of the bowel more watery and helps to flush out any residue. Movicol is a harmless medicine, and frequently used for common constipation. It is often necessary to take movicol for several weeks to completely clear the build up of residue. If the problem is more severe, especially of there is complete blockage of the bowel, treatment will be needed in hospital. Bowel blockage is more common in children who had bowel surgery as babies - in these children, bowel blockage can be caused be adhesions as well as DIOS. CF-related diabetes - CFRD
Testing for CFRDCFRD can come on very slowly. Picking it up early can prevent it from causing problems with weight gain and loss of lung function. This is why we ask all children over the age of 12 years to do a 'glucose profile'. This is where fingerprick blood tests for sugar levels are made a few times per day for 3 days. High levels of glucose (over 10mmol/L) can be a sign of CFRD. Treating CFRDChildren who are suspected of having CFRD will be discussed with the diabetes specialists in the hospital and a treatment plan will be worked out. Treatment will include insulin injections (1-4 injections per day), measuring blood sugar levels with fingerprick tests and some changes to the diet. CFRD is different from typical (type 1) diabetesThe common form of diabetes that can affect any child, and which typically comes on out of the blue, is called type 1 diabetes. In this form of diabetes there is virtually no insulin production. This is a much more dangerous form of diabetes where no having insulin is usually fatal. In CFRD there is still some insulin produced - and enough to prevent these very serious consequences. This is also why the classic symptoms of being very thirsty and passing more urine do not usually apply to CFRD. More informationThe CF Trust has a factsheet on CFRD - download here Coughing up blood - HaemoptysisHaemoptysis means coughing up blood or blood in the sputum. This is usually present due to chronic airway inflammation where streaky blood in the sputum is relatively common. Often this means there is an infection and we will usually want this to be treated with antibiotic. Rarely, larger amounts of haemoptysis can be due to bleeding from larger blood vessels (such as arteries) into the airway. The amount of blood from this can be very variable and this can be very serious and needs urgent, immediate medical attention. A gurgling sensation may be felt in the chest and this can help to give a location for the bleeding. Larger haemoptysis always requires admission to hospital for various investigations and treatment. Physiotherapy may need to be temporarily altered to reduce the chance of worsening the bleeding. Blood from the airway needs to be distinguished from blood from the gut (called haematemesis) but we always want to be informed about any episodes of bleeding. Nasal polypsNasal polyps are benign fleshy growths inside the nose and/or sinuses. Their exact cause is not known but it is thought that they are related to inflammation in the area but there may be other factors involved such as allergy or infection. In CF, polyps are relatively uncommon in children (seen in around 10%) but can occur in up to 40% of adults. They often cause no symptoms if small but larger polyps can cause nasal obstruction or discharge and mouth breathing. They can also cause an impaired sense of smell and taste, as well as chronic sinusitis and headaches. Treatment is usually with a nasal steroid spray, although this can take many weeks to be effective. Surgery is occasionally required but there is a very high recurrence rate and repeat operations are often needed. Liver diseaseLiver problems can occur in a small number of children with CF. The cause of CF liver disease is not well understood, but is probably something to do with bile production by the liver. Bile, made by the liver, is stored in the gall-bladder and released in the gut to aid digestion. We look for CF liver disease every year with ultrasound scans and blood tests. Ultrasound changes of the liver are common in children with CF - upto 60% will show show change in liver echogenicity. Most ultrasound changes are mild and unless they are present for 2 or more years, don't need treatment. Upto 25% of patients can get some scarring in the liver (called cirrhosis) which if it does occur will be present usually before the age of 20 years old. In only a very few children (about 2%) will liver disease lead to signficant health problems. TreatmentIf there are liver ultrasound changes for 2 years in a row, we start a medicine (taken by mouth) called ursodeoxycholic acid. This is a bile salt and it is thought to help the flow of bile through the liver and slow or prevent CF liver disease from getting worse. In the very small number of children with more severe liver disease, we will refer to a liver specialist for advice on treatment. Very, very occasionally a liver transplant may be needed. Stress incontinenceThe involuntary leaking of urine is commoner in people with CF, particularly females (but it does also happen in males). It is particularly likely with coughing, but can also happen with activities such as sneezing, laughing and exercise. The amount of urine that leaks can be anything from a few drops to the emptying of the whole bladder. It can be very embarrassing to talk about stress incontinence and it is often not reported and can sometimes lead to avoidance of coughing and carrying out chest physiotherapy. From the age of 10 all children are asked at annual review if they have any symptoms of stress incontinence. The CF Physiotherapist will teach a programme of exercise to help to strengthen the pelvic floor and a simple technique the knack to practice at home. Advice on posture and core strengthening exercises are also helpful-a separate appointment might be helpful for this to spend more time with your child discussing this. More informationThere is an information leaflet available from the CF trust about the problem - click here The ERIC website can also be helpful - click here Weak bones - low bone mineral density
Why is it a problem?Weak bones can break more easily. Fractures are very rare in childhood, but can happen in adults with CF. Often the bones break are the bones in the spine (verterbra) and the ribs. Both are very painful and make it very had to cough and do physiotherapy. This means lung disease can get worse quite quickly. Prevention is better than cureMost bone mineral is laid down during childhood and teenage years. It is important to start adult life with strong bones, and then work hard to keep them strong. The best way to make sure the bones are stong is to do lots of weight-bearing exercise (ie exercise whilst standing), to eat well and maintain good nutrition and to make sure vitamin D levels are normal (remember to take vitamin supplements with fat containing food and creon). Testing for low bone mineral densityEvery year we measure vitamin D levels in the blood at annual review; we also measure a hormone called PTH. Although we like to have vitamin D levels about 75nmol/L, they can be difficult to interpret on their own. If the body is really short of vitamin D, the PTH level goes up. The combination of a low vitamin D and a high PTH is especially concerning. We write to all families with the results of the vitamin blood test - and make recommendations if necessary. If changes need to be made, they will either be to change the regular dose of vitamin D (usually taken as vitamin A&D capsules or dalavit) or (usually in older chidren) to do this and to have a booster dose of strong vitamin D tablets. In teenagers over 14 years old, we also measure bone mineral density using a DEXA scan (see Bone density (DEXA) scans page). We usually do this only once. The CF Trust suggests that this test is done in all children over 10 years of age, and that it is repeated every 1-3 years. We have not followed this policy since finding very low (-2 z scores) bone density is rare, and the recommended intervention is to do more exercise, check the vitamin D, and optimise the diet - which we should be doing anyway. This are a group of medicines called bisphosphonates which are used in adults, but rarely in children unless there are problems with fractures. More informationThe CF Trust has a factsheet on bone mineral density - download here A more medical document from the CF Trust is also available - download here |
 A quick anatomy reminder helps understand this problem. Swallowed food goes down the food tube (oesophagus) to the stomach. In the stomach the food is broken up and then passed in the small intestine where the nutrients from the food are absorbed. The residue passes into the large intestines (also called the colon) where water is absorbed leaving faeces which are stored in the rectum before being passed. In some children with CF, probably bcecause the intestinal mucous is thicker and stickier than usual, there can be a hold up of material in the last part of the small intestine (sometimes called the terminal ileum). This can lead to the bowel being partly blocked, which can cause tummy ache. Very occasionally the bowel can get completely blocked, resulting in more severe pain and vomiting.
A quick anatomy reminder helps understand this problem. Swallowed food goes down the food tube (oesophagus) to the stomach. In the stomach the food is broken up and then passed in the small intestine where the nutrients from the food are absorbed. The residue passes into the large intestines (also called the colon) where water is absorbed leaving faeces which are stored in the rectum before being passed. In some children with CF, probably bcecause the intestinal mucous is thicker and stickier than usual, there can be a hold up of material in the last part of the small intestine (sometimes called the terminal ileum). This can lead to the bowel being partly blocked, which can cause tummy ache. Very occasionally the bowel can get completely blocked, resulting in more severe pain and vomiting.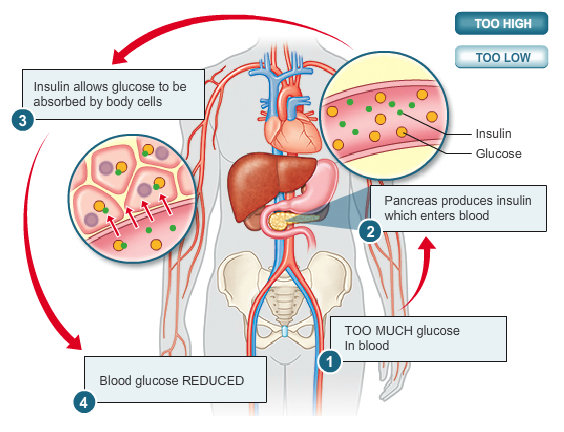 The pancreas is nearly always affected in CF (see 'About CF'). The pancreas has 2 main jobs - to make enzymes to help digest food and to make insulin. Insulin is a hormone that is essential for cells to use sugar (glucose). After we eat food, glucose is absorbed from the gut into the blood stream. Insulin is needed to get the glucose out of the blood and into the cells where it can be used. The pancreas is damaged and scarred in CF - a process which has occurred before the child is born. This means that the pancreas cannot grow as it should. As children get older and bigger the amount of insulin made by the pancreas may not keep up with the demands of a growing body. Not enough insulin means not all the glucose (and therefore energy) from food can be used. This can lead to poor weight gain. High glucose levels in the blood stop the immune system working properly and this can lead to more chest infections and worse lung function. In early CFRD there may be no symptoms, even though lung function may be slipping and weight gain might slow down. CFRD occurs in about 20% of teenagers and 40-50% of adults with CF.
The pancreas is nearly always affected in CF (see 'About CF'). The pancreas has 2 main jobs - to make enzymes to help digest food and to make insulin. Insulin is a hormone that is essential for cells to use sugar (glucose). After we eat food, glucose is absorbed from the gut into the blood stream. Insulin is needed to get the glucose out of the blood and into the cells where it can be used. The pancreas is damaged and scarred in CF - a process which has occurred before the child is born. This means that the pancreas cannot grow as it should. As children get older and bigger the amount of insulin made by the pancreas may not keep up with the demands of a growing body. Not enough insulin means not all the glucose (and therefore energy) from food can be used. This can lead to poor weight gain. High glucose levels in the blood stop the immune system working properly and this can lead to more chest infections and worse lung function. In early CFRD there may be no symptoms, even though lung function may be slipping and weight gain might slow down. CFRD occurs in about 20% of teenagers and 40-50% of adults with CF.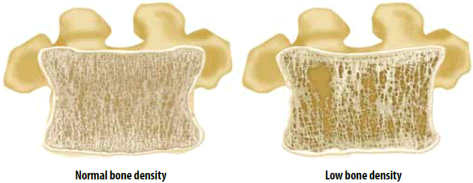 The strength in bones comes from the mineral content - mainly calcium - and the amount of mineral in the bone is called the 'bone mineral density'. Having any long term illness can reduce the bone mineral density. In CF low bone mineral density arises because of a combination of being less active (bone get stronger the more they are used), having a poor appetite and so eating less calcium, and not having enough vitamin D. Treatment with oral steroid medicine, which is sometimes needed in CF, can also weaken the bones.
The strength in bones comes from the mineral content - mainly calcium - and the amount of mineral in the bone is called the 'bone mineral density'. Having any long term illness can reduce the bone mineral density. In CF low bone mineral density arises because of a combination of being less active (bone get stronger the more they are used), having a poor appetite and so eating less calcium, and not having enough vitamin D. Treatment with oral steroid medicine, which is sometimes needed in CF, can also weaken the bones.